


The US' Maternal Mortality Rate
[Trivia: What are the 5 most populous cities in Europe? Hint: 3 of them are in 2 countries not exclusively considered European.]
A while ago I remarked about America’s notoriously high maternal mortality rate and reminded myself to actually look into that at some point.
In a perfect world, there would be a spreadsheet, where every row represented one pregnancy and every column represented every piece of information you could possibly want to know—prematurity, DOB, nation, income level, marriage status, birth order, urbanity of birthplace, etc. etc. And I knew that finding numbers would be hard, because we live in an imperfect world, but I underestimated how hard. Quickly I found myself relying on different people’s write-ups and studies.
Many definitions of maternal mortality seem to try to encompass any death of a mother from during a pregnancy or within one year of the end of the pregnancy (which is usually birth). For example, the CDC notes that they had relied on a list of 25 hospital codes, until 2015, at which point they switched to a revised list of 21 different codes. Obviously, I’d like to find apples-to-apples comparisons, and this is the sort of thing that would make comparing across nations or across time potentially fraught.
Another wrinkle I came across looking at our northern neighbor, Canada. A 2002 study examined Canadian death certificates and concluded that a number of maternal deaths had been under-reported because stillbirths from within the past year had not been noted. They duly re-assessed the figures, looking at 1988-1992. “The officially reported maternal mortality ratio for the study years was 3.7 deaths per 100,000 live births,” the study’s abstract relates. “Depending on whether we included deaths not certified as maternal deaths at the time the deaths occurred, revised ratios under ICD-9 ranged from 4.9 to 5.1 per 100,000 live births for deaths from direct obstetric causes and from 0.5 to 1.2 per 100,000 live births for deaths from indirect obstetric causes.”
Now, going through write-ups, it wasn’t hard to find motivated reasoning. (I’d expected as much.) The CDC, for instance, charted mortality rates by ethnicity and remarked,
Variability in the risk of death by race/ethnicity may be due to several factors including access to care, quality of care, prevalence of chronic diseases, structural racism, and implicit biases.
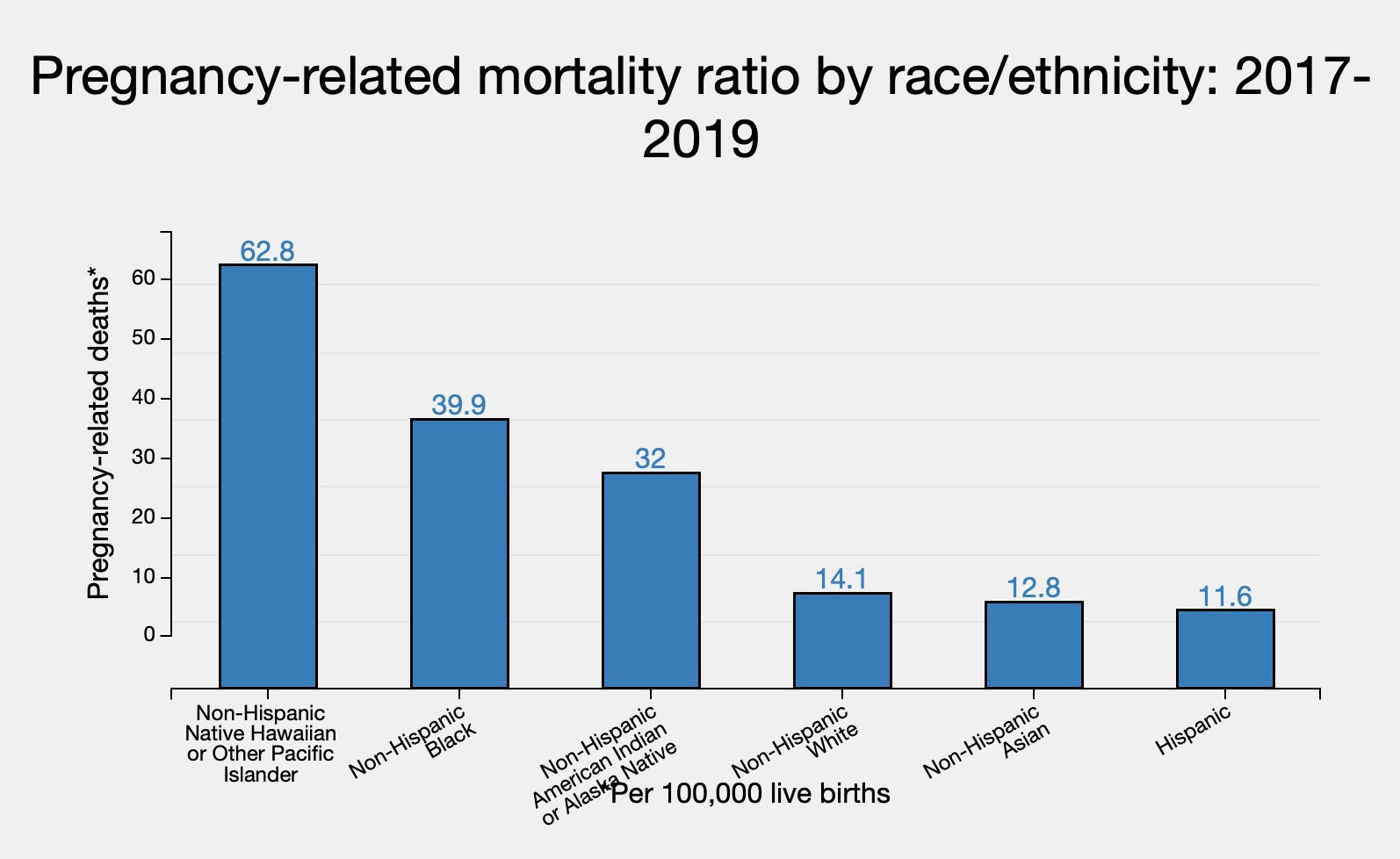
This chart. It always catches my eye when a statistic ranks Americans in the order “Hispanic, Asian, White, Black.”
Meanwhile, there’s Deseret News, which is an outlet based in Utah and run by the Mormon Church. They ran a piece that highlighted the following:
Why are so many of our mothers dying?
Researchers have suggested personal health factors, such as higher rates of obesity and diabetes, may be a factor in these rising maternal mortality rates. That is no doubt true, but there is a deeper and more disturbing explanation: homicide.
In a stunning new study amplified recently in Nature, and originally published this month in Obstetrics and Gynecology, Maeve Wallace of Tulane University and several co-authors find that homicide is the leading cause of death of pregnant women.
. . . It’s also important to ask how many of these homicides occurred because the woman refused her partner’s request to abort the child.
Then the piece takes a pretty weird turn.
There are numerous cases where this has in fact been the motivation for the murder of a pregnant woman, and it brings us to a critical point of discussion. Every proposed legal ban or partial ban on abortion has always included an exemption where the life of the mother is in jeopardy. When we hear that exemption, we are no doubt thinking of the woman with pre-eclampsia or hemorrhage who will die without an abortion. Do we ever think of the women who will be murdered without access to abortion or who will be murdered because they refused an abortion? Shouldn’t both these situations be part of the policy debate?
If homicide is indeed the single largest cause of death among pregnant women, then that simple fact suggests that they should. Policymakers should take this opportunity to fill the gaps and ensure women faced with this situation actually can get the help they need.
I’m not sure where the author—a professor at Texas A&M’s School of Government—really thinks where this argument is supposed to go. The first thought sounds like caving to terrorists; the second part sounds completely out-of-the-box. What policy solution is there for a woman who faces murder if she refuses an abortion? Would that possibility be addressed by some sort of communication between police and public health systems? Or is the point trying to be made here about being more permissive with abortion policies—it’s an enormous head-scratcher.
Intriguingly, the study cited comes from Tulane University, based in New Orleans, Louisiana, which is among the worst US States along the maternal mortality metric. That university also (in 2021) put out a pretty unabashed piece of agitprop entitled “Study finds higher maternal mortality rates in states with more abortion restrictions.” Now this is just moonshine. Here’s the map:

Now, I’m not sure what metric puts Virginia, Louisiana, and Idaho in the same tier of abortion restriction bhp Nevada, Wisconsin, and Massachusetts together in a different one. I’m also not sure how something like this could pose as serious research given the obvious factor that wealth is going to play (and what that looks like across this map). Now, I couldn’t find maternal mortality rates differentiated by income. But I can’t believe that that’s not relevant. But anyway, this study went ahead to write:
“It is critically important that state-level policies related to women’s access to comprehensive reproductive health care services, including abortion, are evidence-based and guided by the primary goal of improving women’s health and reducing maternal mortality,”said Dovile Vilda, research assistant professor at the Department of Social, Behavioral and Population Sciences and a lead author on the study. “Our study provides evidence that decreasing the number of abortion restrictions across the states may reduce incidence of death during pregnancy and postpartum among all women in the US.”
But as far as what’s actually driving US maternal mortality rates that (1) apparently are high compared to other comparable nations, and (2) apparently are increasing—I’ve seen a couple different explanations. Higher ages of childbirth showed up, as did a lack of training and best practices on maternal (rather than infant) care, and a unique failure for American mothers to address chronic health issues prior to pregnancy.
Now obviously, I want actual numbers on things. One NPR write-up (from 2017)
Meanwhile, life-saving practices that have become widely accepted in other affluent countries — and in a few states, notably California — have yet to take hold in many American hospitals. Take the example of preeclampsia, a type of high blood pressure that occurs only in pregnancy or the postpartum period, and can lead to seizures and strokes. Around the world, it kills an estimated five women an hour. But in developed countries, it is highly treatable. The key is to act quickly.
By standardizing its approach, Britain has reduced preeclampsia deaths to one in a million — a total of two deaths from 2012 to 2014. In the U.S., on the other hand, preeclampsia still accounts for about 8 percent of maternal deaths— 50 to 70 women a year.
(Bolding mine.) They never actually gave two directly comparable numbers there, so my rough estimate for you is: if “one in a million” does indeed mean one / 1,000,000 births, then, figuring on the US having roughly 4,000,000 births per year for that time frame and around 60 fatalities from that one cause, that means there’s about a 15-in-a-million chance of that cause of death. 15 times worse.
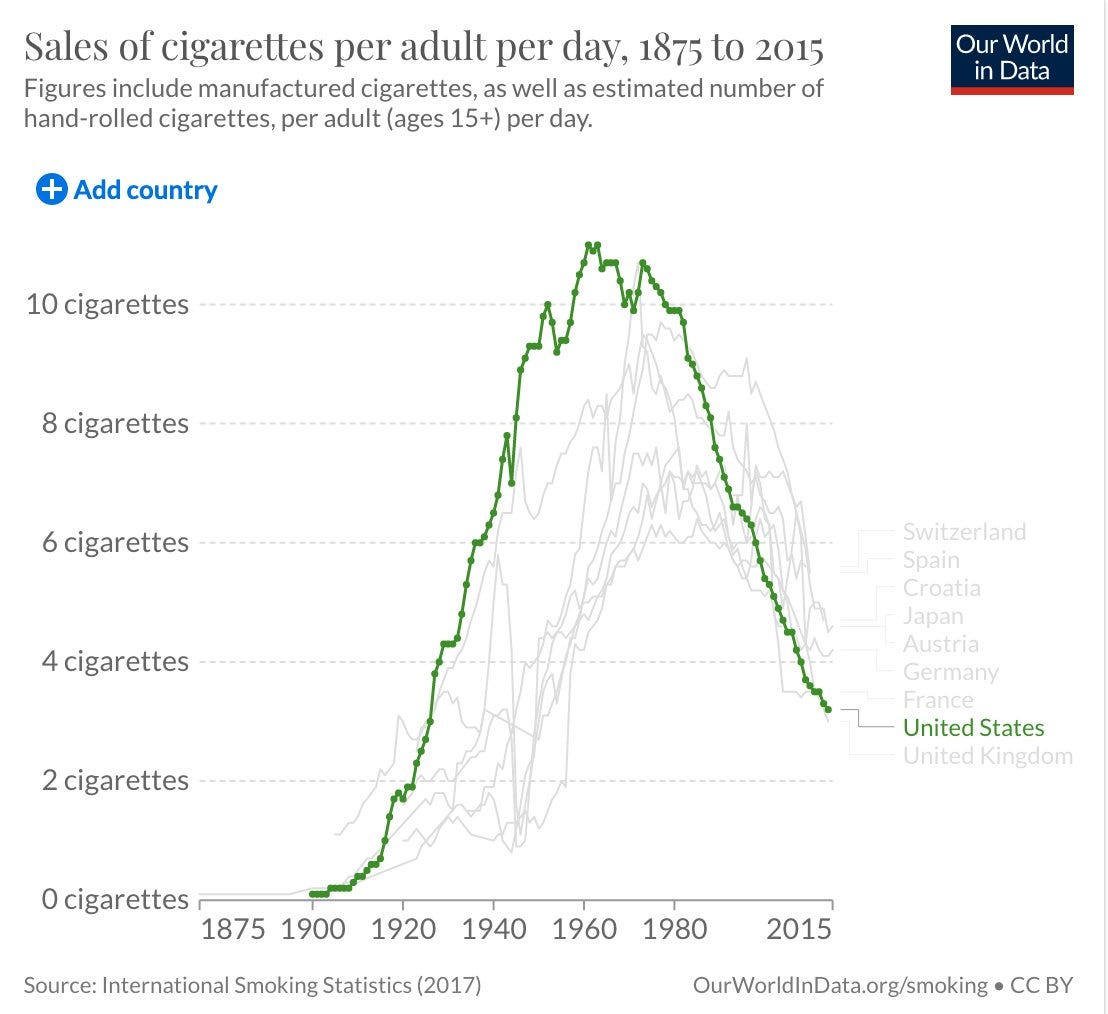
But like I said at the beginning, mostly I’m overwhelmed by this complexity. This phenomenon might just be true and just another outgrowth of what one person (in the context of smoking) called American exceptionalism, “for better and worse.”
~
Answer: Istanbul, Moscow, London, St. Petersburg, and (the biggest in the EU) Berlin.